It deals with endocrine problems that occur in children. Apart from growth disorders, Thyroid and diabetes mellitus are also common. Children also suffer from a spectrum of pubertal disorders such as precocious puberty to delayed puberty. Obesity is now more common in children.
Common Disorders:- Short stature
- Delayed puberty
- Precocious puberty
- Abnormal breast development in children
- Childhood obesity
- Type 1 diabetes
- Thyroid problems
- Rickets

Physical growth of children is always a subject of talk among their parents, grandparents and caregivers. Your kid’s growth is normally compared with their peer group like siblings, classmates or playmates. Parents are very worried if their child is not growing according to his/ her age and falls short of his/her expected height (Short stature). Short stature also becomes a psychosocial issue due to lack of self-esteem in a growing era of peer pressure. But seeking prompt medical help is the key to appropriate investigation, early diagnosis and initiation of treatment. Unfortunately, most kids are brought to us late for evaluation and treatment is not possible or results are poor. If you are worried about your kid’s height, please ensure that they see an endocrinologist 3-4 years before puberty (7-8 years in girls and 9-10 years in boys).
The common causes of short stature include:
- Growth hormone deficiency.
- Familial short stature.
- Hypothyroidism.
- Syndromic causes like Turner syndrome.
- Nutritional deficiency.
- Skeletal dysplasias and Rickets etc.
- Chronic use of steroids.
- Chronic illnesses like renal, respiratory, cardiac, renal or gastro-intestinal problems.
Evaluation of a child with short stature includes a detailed recording of history, review of height and weight recordings over the previous few years, accurate measurement and documentation of height, weight, mid parental height, target height, growth velocity, head circumference, arm length, assessment of nutritional status, systemic examination, assessment of pubertal status and bone age.
Role of Endocrinologist in the evaluation of short stature includes identification of the cause, providing nutritional counseling and psychological support to the family and judicious use of latest hormone therapy in improving the height of the child. An Endocrinologist plans and conducts dynamic hormone testing to assess the response of Growth hormone (Growth hormone stimulation test) which is secreted from the Pituitary gland of the child. Growth hormone stimulation test is done by various methods like Clonidine stimulation test, Insulin Tolerance test, Glucagon stimulation test etc and a suitable test is selected depending on the particular individual’s need. Meticulous planning, repeated blood sampling at timed intervals (30 mins, 60 mins, 90 mins and 120 mins etc.), monitoring the vital parameters of the child during testing (BP, Sugars) and above all thorough knowledge about the interpretation of the results is mandatory. As Endocrinologists have a clear understanding of all these issues, we are able to manage short stature with a holistic approach.
Once a proper diagnosis of Growth hormone deficiency (GHD) is established or a cause for short stature is established treatment becomes easy. Growth hormone therapy has revolutionarized the management of short stature in Growth hormone deficiency. It is really a boon for a short child who will otherwise become a short adult and will have metabolic, physical and psychological problems related to growth hormone deficiency. It is currently a widely accomplished treatment all over the world and is the standard of care in GHD. Unfortunately, in our country growth hormone treatment is still beyond reach of many needy children because of its cost. But the enormous benefit obtained because of its use with the established safety profile makes it the best option for short children as well as their parents. Most of the children with short stature can be effectively treated and can have improvement in their final height provided they are treated at an early age.
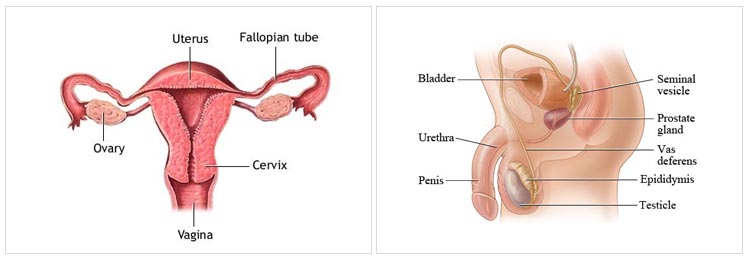
Puberty is a natural process which occurs in a boy or girl during their adolescent age group. The changes culminate in the development of secondary sexual characters, complete physical and psychological development, personality development and ability to procreate. Though the physical changes indicating onset of puberty is generally noticed at around the age of 9-11 years in girls and 10-12 years in boys, the hormonal changes usually precede physical changes by 2 years. For a timely onset and smooth progression of puberty, we all need a normally functioning Hypothalamus (which is present above the Pituitary gland and controls it), Pituitary gland, Thyroid gland, Adrenal glands and the Reproductive organs (testis in male and ovaries in female). Normal puberty is a complex interplay of genetic, hormonal, neural, nutritional and environmental factors. At the end of puberty a boy or girl transform themselves into an young man or woman.
For some unfortunate children, this natural process either does not take-off at the right time or does not proceed to its logical conclusion as expected. We call this as “Delayed Puberty”. The child and their parents will be naturally worried if they do not find physical changes of puberty at an expected age. This has an adverse effect on the self-esteem of the child who finds him/ herself more “boyish” or “girlish” when their peer groups are becoming “adults”.
Parents seek medical opinion from their pediatrician, gynecologist or family physician. About 20-30% of the children seeking medical attention for delayed puberty need careful follow-up and re-assurance alone. Onset of puberty may occur a little later in them but it will progress normally without the need of any treatment. We call this group of children as having “Constitutional delay in puberty”. Treating this group of children with hormone tablets or injection is unnecessary and may increase the financial burden and add up to their parenteral anxiety. On the other hand, there are a number of children for whom timely hormone therapy is necessary or else they will not have puberty and will have “hypogonadism” (low sexual function). An Endocrinologist will be able to differentiate between the two groups with the help of clinical evaluation and hormonal test reports. Children with delayed puberty require thorough evaluation with estimation of bone age and hormone estimation (FSH, LH, Prolactin, Thyroid function test, Estradiol, Testosterone etc.). The doctor may also order an ultrasound scan of uterus and ovaries, MRI scan of Pituitary and genetic testing (Chromosomal analysis) as and when required.
Hormonal therapy for delayed puberty includes 1. Medicines to improve secondary sexual characters (hair growth, breast development, development of genitals etc.) and 2. Medicines to increase sperm production in male or ovum formation in female. Apart from this, the underlying cause for the delay should also be treated. With regular treatment and periodic follow-up, the child can realize his /her dream of becoming a grown up adult.
A mother or grandmother would be really worried if they find their daughter or grand-daughter showing signs of breast development or menstruation at a tender age of 6 years. The tremendous psychological impact the child will have and the worry of her safety in the era of growing child abuse will give them sleepless nights. Incidents of early puberty (before 8 years in girls and 9 years in boys) are not uncommon as there is advancement in the age of onset of puberty worldwide. This secular trend in the occurrence of early puberty is related to increasing incidence of childhood obesity and environmental factors like increased processed and packaged food intake. Nevertheless, early or precocious puberty is a cause of concern because of three important reasons:
- Precocious puberty may sometimes be due to a serious disorder like a hormone secreting tumor in the area of hypothalamus & Pituitary or in the reproductive organs. Failure to identify this problem may lead to long term adverse events.
- A child with precocious puberty will be a tall early but ultimately becomes a short adult later. The sex hormones which are secreted earlier in this child will complete the bone growth quickly. Hence, the child’s final height will be very much lesser when compared to a child of the same age who attains puberty at appropriate age.
- Child with precocious puberty will not have enough psychological development to understand the physical changes happening to her. He or She will still be a “Child” at heart with an “Adult” body. This will lead to adjustment problems, problems with inter personal relationship among peer groups and psycho-social issues.
It is therefore necessary that any girl with pubertal changes before 8 years or boy before 9 years should be brought to medical attention. Hormone evaluation and bone age estimation are imperative to assess the stage of sexual development. Endocrinologists also do dynamic hormone testing called “GnRH stimulation test” or “Leuprolide stimulation test” in these children to see if the source of excess hormone is from the pituitary or from other site (ovaries or testis). Appropriate scanning (MRI of pituitary, Ultrasound of testis or ovaries) are the next line of tests once the source of hormone excess is confirmed in blood tests.
After diagnosis, treatment can be started to slow down the progression of puberty till the normal age of pubertal development (11-12 years). Effective medicines are available which may be used once in 3 months to get the desirable results. Periodic monitoring of hormone levels is essential during the treatment period. This treatment has an established good safety profile with no significant long term side-effects. Once the treatment is stopped, the child can resume a normal puberty at the right age without any hurdle. He or she will also have a significant height gain during this period as rate of bone growth is normalized from its rapid pace. Also the apprehension of the child as well as the parents can be relieved which leads to psychological well-being.